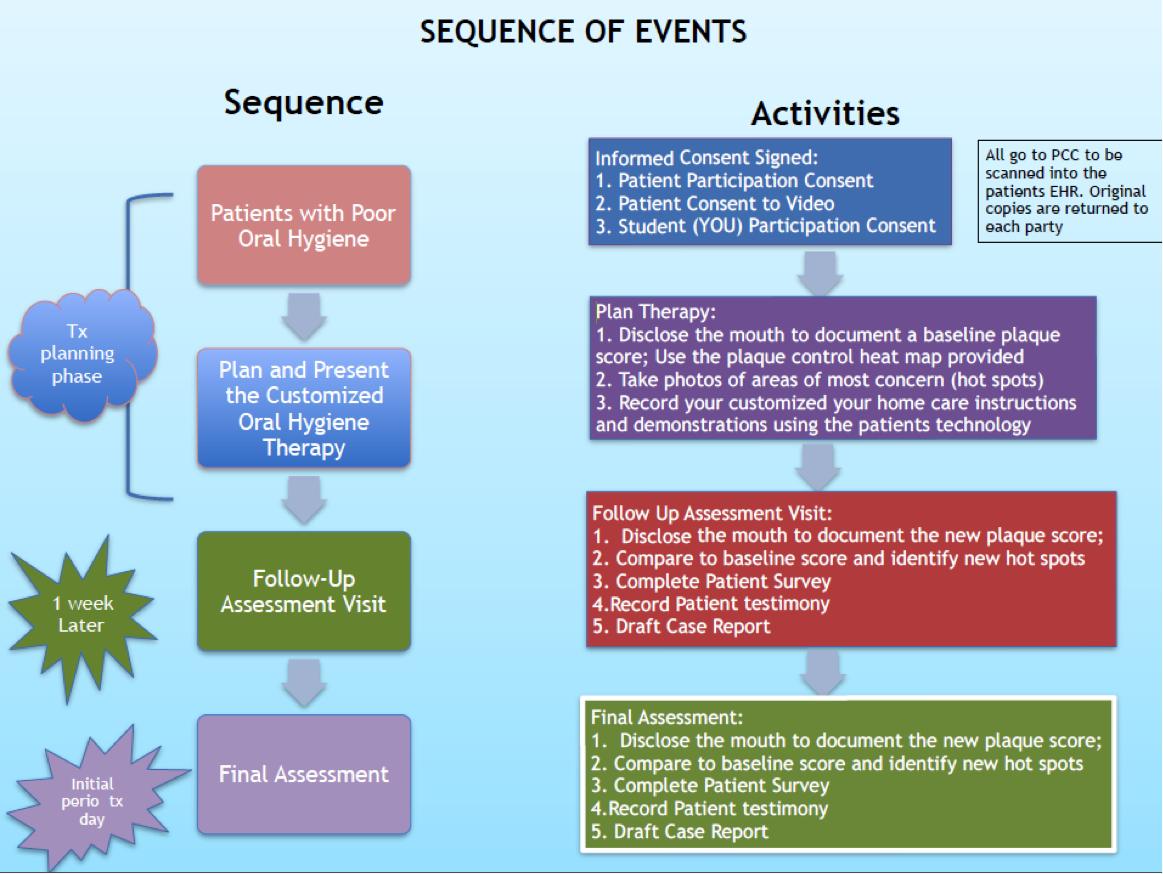
Oral hygiene therapy (OHT) may be one of the most challenging treatments because patient education is critical to encourage life-long changes in patients’ oral care habits. We believe that customizing OHT has great potential to improve patient outcomes. This case submission competition will encourage students to creatively engage in COHT with their patients, and share their results with faculty.
Students will engage their patients in customized oral health therapy (COHT) and write a report detailing the methods they used. This report will include text, plaque control records (or heat map), photos, and optionally supported with video of the patient interaction or demonstrations of OHT techniques on the patient.
Submissions will be tracked according to VICs clinic (2 Green, 3 Blue, etc.). The clinic scoring the most total points by Oct. 21, 2016 will win a clinic-wide pizza party! Individuals may submit more than one case.
The following rubric will be used to judge each case submission.
All submissions must have background, heat maps, teaching patients how to use oral aids, and surveys. Optionally, you can add teaching media and data from a recall appointment for bonus points. The more details you put into it, the more points your case receives= more points for your clinic= better chance of pizza party :)
View the rubric to see all the possible criteria. Remember - the KEY to successful periodontal therapy is efficient home care by a motivated individual!
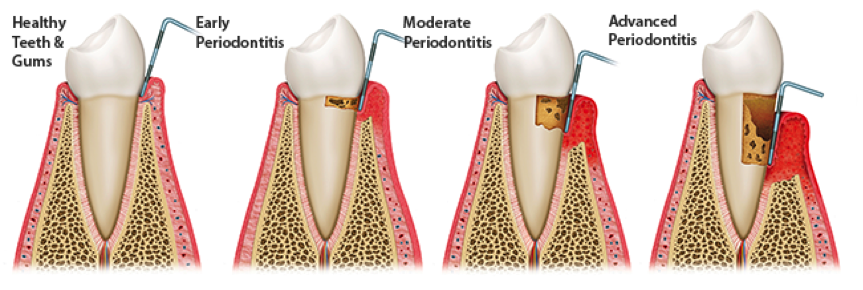
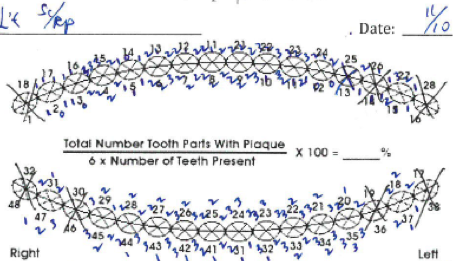
A 55-Year-old Male reported to the VIC clinic with the chief complaint of Malodor. Comprehensive oral examination and complete periodontal chart was performed. Localized moderate chronic periodontitis is diagnosed and initial comprehensive periodontal therapy is proposed to the patient, including mini-quadrants of scaling and root planning, controlling systemic & local factors, and oral hygiene therapy. The gingiva showed localized erythema, blunted papilla, and rolled margins. The Plaque remnants were visualized with disclosing agent such as Bismarck brown (Fig.1A). Patient received oral hygiene therapy over several visits during the initial periodontal therapy (Hygienic phase); local factors associated with the hot spots were also identified, including caries on #10 (D) and overhanged composite restorations were seen on #11(D) (Fig 1C). See patient demo video that easy flosser get stuck and broken off due to the cavity margin on tooth #10 (D) (Video 2).



We explained to the patient that malodor is multifactorial and there are different contributing sources, including periodontal disease, oral hygiene, respiratory and digestive tract. Suggest the patient to drink green tea and also proceed with periodontal disease treatment.
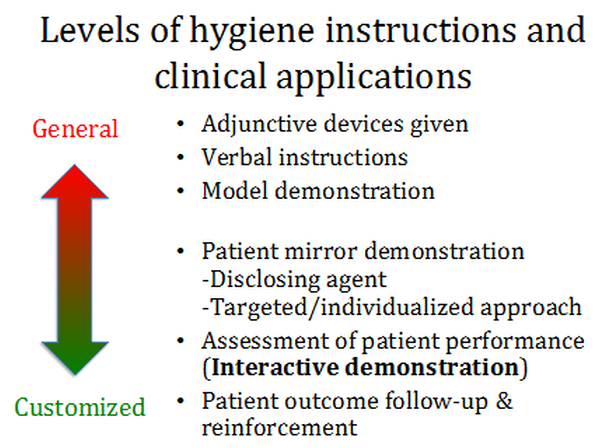
Etiology of the periodontal disease was explained to the patient for motivation and oral care behavioral change. Utilization of visual aid in the consultation visit for patient education and this will help patients understand what’s happening and why targeting gum line. The patients will also appreciate why periodontal charting (probing) needs to be done.
Significant generalized plaque accumulation, but due to the time constraint, verbal oral hygiene instructions were given.
“You need to brush two times a day and floss”
“You need to angle your brush toward the gum”
During the periodontal record presentation, systemic factors (immune system, smoking, DM, nutrition) as well as local factors (caries and defective restoration, see the following progress) were also discussed with the patient (Could be done during the initial visit). Patient was disclosed and plaque control heat map was recorded before the scaling and root planning.
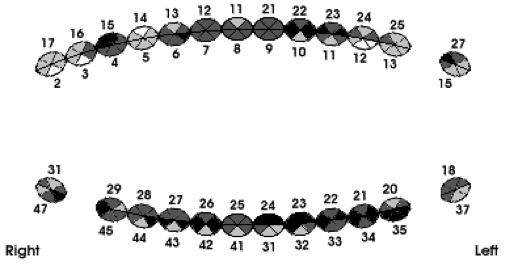
Conversion of analog heat map to gray scale:
Customized Oral Hygiene Therapy
A combined Bass and Fone’s technique was demonstrated to the patient. It is interesting to see that each technique has its specific efficiency over certain surface and plaque accumulation pattern. It seems that Bass method is more efficient on midbuccal cervical areas and Fone’s technique (vertical circular) can get into the embrasure area more effectively. Therefore we combined both techniques and instructed the patient to brush 3 secs for each methods for the a total of 6 secs per area.
Since the patient never floss, we started instructing easy-flosser (Fig 2) to begin and focusing over #10 & #11 area. Please see Video 1 & 2 regarding the demonstration and patient’s repeat exercise. The video was sent to the patient for at-home review.
During the initial periodontal therapy, as part of the comprehensive treatment, local factors were also removed. Composite restoration of #10(D) caries was done and adjustment of overhang at the distal-lingual line angle of tooth #11 with the polishing strip. After controlling the local factors, the patient was able to use flosser more easily and the area is better maintainable without these plaque retentive factors (Fig 3).



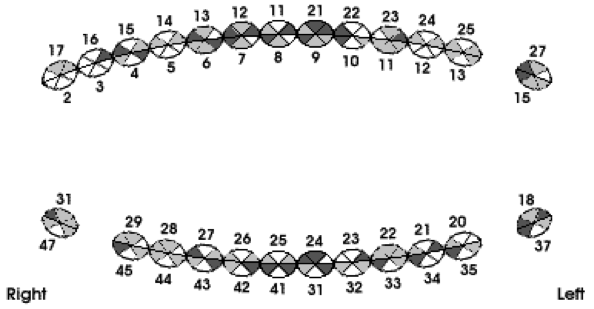
Generalized improvement in terms of plaque index on most of the surfaces. Although there is not a specific improvement “pattern”, more targeted approach can still be implemented. End-tufted brush for distal of the premolars and isolated molar was demonstrated (Video 3 & 4). Given that most surfaces with plaque index of 2 were still mostly interproxinally, we reinforce the easy-flosser. We also asked the patient to brush well before coming in next visit.
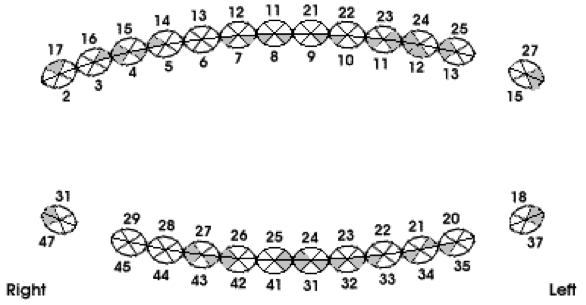
Significantly improved was noted after plaque control heat map was recorded. There is no plaque index of 2 areas. Very minimal and thin plaque at the interproximal or embrasure area. Localized periodontal pockets reduced from 6 to 4 mm with no bleed upon probing. Patient also self-reported that the malodor improved significantly resolved.
| Plaque Score 3 | Plaque Score 2 | Plaque Score 1 | Plaque Score 0 | |
|---|---|---|---|---|
| First visit | 37 | 68 | 40 | 5 |
| Final visit | 0 | 0 | 42 | 108 |
In addition, other oral hygiene devices such as tongue scrapper for cleaning the tongue was also introduced to the patient (Fig 4) at the initial visit.

One of the challenges is that the video may be too big to send it through email. But after some minor editing with iMovie, using different format can reduce the file size a lot.
Patient thought that his oral hygiene is ok and brushes once a day. He received the videos through cellphone and watched the video once and found it helpful. After COHT, he brushed twice a day with the easy flosser – in an effective way! He feels his oral hygiene is good and feels more energetic afterwards. He strongly recommends this therapy to other patients.
Provider demo for easy-flosser
Patient repeat exercise (easy-flosser)
Provider demo for end-tufted brush
Patient repeat exercise (end-tufted brush)
Is it really easy?
What is the problem in this video demonstration?
Do you know how the interdental brush sometimes needs to go from the lingual side?
This is the place to to submit your Customized Oral Hygiene Therapy intervention success stories. All submissions due by Midnight Oct 21, 2016. You may submit more than one case.

(Left to right) Dr. Jeff Wang, Barjinder Takra, Vaishnavi Bhaskar, Panchali Patel, Kanchi Shah, John Zona, Peter Liang, Sydney Sherman (in spirit)
.JPG)
(Left to right) Dr. Jeff Wang, Barjinder Takra, Vaishnavi Bhaskar, Panchali Patel, Kanchi Shah, John Zona, Peter Liang, Sydney Sherman (in spirit)
Recipient: Vaishnavi Bhaskar
(Left to right) Vaishnavi Bhaskar, Dr. Jeff Wang
Department of Periodontics and Oral Medicine
School of Dentistry
University of Michigan Ann Arbor
1011 N University Ave
Ann Arbor,MI 48109